
Translate this page into:
Can response time be trained with bilateral limb training in children with Down syndrome?
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Aims:
Response time (RT), that is, the time taken to respond is known to be delayed in children with Down syndrome (DS). We performed a pilot study to evaluate whether bilateral limb training can be used to train RT, in children with DS.
Settings and Design:
10 children with DS (5 males) were recruited from a special school in a suburban region using convenience sampling.
Subjects and Methods:
Response time was measured using an indigenously developed RT Analyzer, before and after intervention, from right and left hand. Structured bilateral limb training was given for a period of 4 weeks, using low-cost, locally available materials, in community settings.
Statistical Analysis Used:
The Wilcoxon signed ranks test was used for statistical analysis.
Results:
Significant improvements in RT following 4 weeks of intervention were seen in the left hand (P = 0.006) but not in the right hand (P = 0.104).
Conclusions:
Response time can be trained in children with DS using 4 weeks of bilateral limb training activities using low-cost, locally available materials.
Keywords
Bilateral limb training
community-based rehabilitation
feasibility
low-cost materials
pediatric rehabilitation
training

Introduction
Children with Down syndrome (DS) are known to have dysfunctions in motor control which lead to deficits in fine and gross motor skills.[12345] These dysfunctions are accompanied with an increased time to learn skills and a tendency to be slow while performing movements.[56]
Ability to respond to a stimulus is a basic component of our daily living. The time taken to respond to a stimulus is termed as response time (RT).[7] This time includes the time taken from the perception of the stimulus to the initiation of a response and the initiation of response to the completion of the action.[8] Short RT is essential to perform an activity quickly and efficiently. Increase in RT leads to slowness, clumsiness, and invariably has an effect on performance of skilled activities, dynamic balance, and agility.
In comparison to healthy individuals, lower and variable RT has been observed among individuals with DS.[79] A study done by Marzi et al. showed that there is a 300 ms delay between RT of adults with DS and age-matched healthy controls.[10] When compared with typically developing children, children with DS demonstrate slowness of movement during play activities, like one handball-catching.[11] Dysfunctions in the temporal components of motor tasks could be responsible for the slowness in the timing of movements in DS.[12]
Studies show that children with DS have a huge potential to improve their motor performance.[1314] Rehabilitation in children with DS mainly aims at improving strength and postural control. However, training to improve RT has not been well-studied. Previous studies in individuals with moderate and severe intellectual disability have found that training helps improve response and movement times.[1516] Structured physical fitness program has shown an improvement in RT abilities of children and adolescents with intellectual disability without DS.[17] Similar forms of exercise training which aim at training to improve RT in children with DS have not been explored.
Studies show that the corpus callosum, which provides a channel of communication between the two hemispheres, is anomalous in individuals with DS. This could be the reason for the increased interhemispheric transmission time, that is, the time required for the transmission of impulses from one cerebral hemisphere to another, seen in individuals with DS.[1018] The increased interhemispheric transmission time could be one of the reasons for the slower RT seen in DS. Activities which help activate both hemispheres alternately or simultaneously may improve the communication between the hemispheres, which may reduce interhemispheric transmission time thereby improving the RT. Since bilateral limb training is known to activate both hemispheres,[19] we hypothesized that structured bilateral limb training could help improve RT in children with DS. The study aimed at evaluating whether training with bilateral activities can improve RT in children with DS. The study also aimed at evaluating if this training can be achieved using low-cost, locally available materials in community settings.
Subjects and Methods
Design
A quasi-experimental, pretest-posttest design, was used to evaluate the influence of training on RT. Data were collected before and after 4 weeks of intervention.
Participants
The participants were recruited from a special school in a suburban region. Children with DS, aged between 9 and 17 years, who were functionally independent and able to understand and follow one step command, with corrected vision and hearing, were recruited for the study based on convenience sampling. Children who were uncooperative or had any associated medical condition which could interfere in their exercise performance were excluded from the study. Of the 17 children with DS, 10 children (5 males) met the inclusion criteria of the study.
Instrument
Response time was measured using an RT Analyzer which was indigenously developed. The instrument had the components of a light stimulus and a hand switch. A digital timer was a component of the instrument which measured the time interval between the appearance of the light stimulus and pressing of the switch. The analyzer was calibrated, its accuracy was tested and its test-retest reliability was measured, by the same procedure as stated below, prior to the commencement of the study. The test-retest reliability of the RT analyzer was tested among 17 adults between the age of 20 and 25, was found to be good reliability for both the extremities, that is, right hand (intraclass correlation coefficient [ICC] = 0.922) and left hand (ICC = 0.878).
Procedure
Permission to conduct the study was obtained from the administrator of the school along with consent from teachers/guardians and assent from participants. The study was conducted in full accordance with the guidelines of the Helsinki Declaration. Assessment of RT and the training was carried out in an isolated room within the school premises.
Response time assessment
The child was seated on a chair with arms supported such that the upper limb could comfortably reach the hand switch placed on the table. The child was asked to keep his/her index finger on the hand switch. The participant was instructed to press the hand switch as soon as the light stimulus appears. The time duration between the appearance of the light and the pressing of the switch was considered as RT. Familiarization of the testing procedure was done for all participants one at a time. Once the participant was familiar with the testing procedure, RT was measured for one child at a time. The examiner presented the stimulus by pressing a switch at different intervals of time ranging from 1 to 5 s. From each participant, in all 20 measurements were taken, first 10 measurements from the right hand and next 10 from the left hand. Measurements were taken at the baseline and again after 4 weeks of intervention.
Intervention
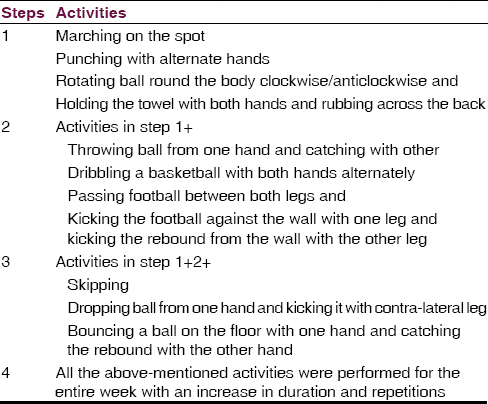
Children were trained with a set of bilateral limb activities, thrice a week for a period of 4 weeks. Simple and cost-effective materials such as towel, softball, football, basketball, and skipping rope, were used for training. The bilateral limb activities were divided into four steps [Table 1]. Each step was added as the intervention progressed to the next week. The training sessions were individualized and supervised, and were performed for an average duration of 45 min. As the activities were taught to the participants, initially repeated feedback was given which was gradually withdrawn as the participants mastered the activities. Routine physical activities were continued for the children during the study period.
Data analysis
Data were analyzed using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). The data were assessed for normality using the Shapiro–Wilk test. Since the data were not following normal distribution, the statistical analysis was done using Wilcoxon Signed Ranks test. The level of significance was set at P ≤ 0.05.
Results
Of the 17 children screened, 12 matched the inclusion criteria, but only 10 children agreed to participate in the study. The flow of participants in the study is described in Figure 1. There was no loss to follow-up and all 10 participants between the ages of 9 and 17 (median age = 14), all right-hand dominant, were included in the final analysis.

- Progression of the study
Change in response time (ΔRT)
Following 4 weeks of intervention, RT improved in both extremities, however, a statistically significant (P < 0.05) improvement was seen in the left hand (P = 0.006*) but not in the right hand (P = 0.104). The change in median values of RT pre and post-intervention is shown in Figure 2. RT improved in the right hand by ΔRH = 502 ms and left hand by ΔLH = 634 ms. The change in RT had no difference when comparison was made between genders.

- The change in response time pre- and post-intervention
Discussion
The study is one of the first attempts aimed at improving RT in children with DS using bilateral limb training in suburban community settings. The study helps elucidate innovative community-based interventions to rehabilitate aspects of RT in children with DS. The study evaluated whether RT can be trained with bilateral limb activities in children with DS using low cost locally available materials in community settings. The results of the study show that bilateral limb training helped improve RT in children with DS.
A number of possible mechanisms could have led to the change in RT. Prolonged practice of a simple motor task in adults with DS has shown improvements in the timing of movement during tasks.[13] Studies in adults with moderate to severe intellectual disability, who were trained using an aiming task, have shown to reduce RT and movement time of the task performed.[1516] Both studies were performed in adults with intellectual disability, and they had a shorter period of training than the present study. Unlike the previous studies where the training focused on aiming tasks and on practicing different movements repeatedly; the present study used task-oriented bilateral limb activities. The result of the present study supports and adds further evidence to already existing literature that training can bring about an improved ability to respond in children with DS. Motor learning and exposure to a different set of activities, in addition to the routine physical activities, could have also led to the change in RT. The initial RT of children was found to be longer. However with bilateral arm training, for a period of 4 weeks, their RT improved. The improvements in RT, however, were statistically significant in the left hand but not right hand. The reason for this could be that the hand from which the measurements were first taken was not randomized. Hence, all the measures were first taken from the right hand and then from the left hand. By the time 10 measurements from the right hand were taken, learning of the task may have led to better response when measurements were taken from the left hand. Randomizing the hand from which the initial was measurement taken could have eliminated this finding. The other reason for the statistically significant improvement in RT in the left side could be because the baseline RT values were more in the left hand. Hence, the overall change was found to be statistically significant only in the left side. We found that the median change in RT (ΔRT), showed improvement both in males and females. Hence, it can be stated that the change in RT is not gender specific.
The training sessions were enjoyed by the children, and there were no dropouts in the study. Since the training was individualized, any absenteeism from school was given the missed session separately. The training was easy and performed using low cost locally available materials within the school premises thereby making the training feasible. Hence, it can be conveniently incorporated in the regular rehabilitation services. The activities were simple enough to be taught to parents, as a home-based program especially during school vacations, to maintain the effects of training.
The main limitation of the study is that the absence of a control group makes it difficult to determine whether the improvement in RT was solely due to the training given. Since all the participants of the study were right-hand dominant, we could not determine the influence of hand dominance on RT. The small sample size makes the findings of this study prone to type II errors. A follow-up period could have helped us understand the carry-over effects of the training. The study if performed with a stricter methodology and a larger sample size may provide us stronger evidence.
Future randomized controlled trials with large sample size can be conducted to assess the effects of bilateral limb training on RT. Future studies can also analyze whether training RT brings about any improvement in function, activity, and participation of children with DS. This would help us better understand the clinical significance of the training program.
In summary, bilateral limb training improves RT in children with DS. Such training is feasible in community settings and can be conducting using simple, inexpensive, and locally available materials.
Acknowledgment
We would like to thank Mr. Manikandan N. for his support with the RT Analyzer and Mr. Manikandan N. and Mr. Abraham Samuel Babu, for their help in proofreading the paper. We would also like to acknowledge the teachers and children from the Special school where the research was conducted.
Ms. Pratiksha Tilak Rao is supported by a 3 years fellowship under the structured PhD program of Manipal University, Manipal, India.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Performance of retarded children, with and without Down syndrome, on the Bruininks Oseretsky test of motor proficiency. Phys Ther. 1986;66:344-8.
- [Google Scholar]
- Specific motor disabilities in Down's syndrome. J Child Psychol Psychiatry. 1974;15:293-301.
- [Google Scholar]
- Motor control in Down syndrome: The role of adaptation and practice. J Dev Phys Disabil. 1992;4:227-61.
- [Google Scholar]
- Gross motor skill acquisition in adolescents with Down syndrome. Downs Syndr Res Pract. 2006;9:75-80.
- [Google Scholar]
- Gross motor function of children with Down syndrome: Creation of motor growth curves. Arch Phys Med Rehabil. 2001;82:494-500.
- [Google Scholar]
- Deficits in the production of grip forces in Down syndrome. Dev Med Child Neurol. 1988;30:752-8.
- [Google Scholar]
- Supra-maximal effort and reaction and movement times in a non-compatible response time task. J Sports Med Phys Fitness. 2005;45:127-33.
- [Google Scholar]
- Choice reaction time: Basic concepts. In: Welford AT, ed. Reaction Times. New York: Academic Press; 1980. p. :73-128.
- [Google Scholar]
- Is interhemispheric transfer of visuomotor information asymmetric? Evidence from a meta-analysis. Neuropsychologia. 1991;29:1163-77.
- [Google Scholar]
- A comparison of time characteristics in ball catching between children with and without Down's syndrome. Acta Univ Palacki Olomuc Gymnica. 2010;40:61-7.
- [Google Scholar]
- The motor deficit in Down's syndrome children: A problem of timing? J Child Psychol Psychiatry. 1981;22:233-45.
- [Google Scholar]
- Practice and transfer effects during fast single-joint elbow movements in individuals with Down syndrome. Phys Ther. 1994;74:1000-12.
- [Google Scholar]
- Learning motor synergies by persons with Down syndrome. J Intellect Disabil Res. 2007;51:962-71.
- [Google Scholar]
- Training moderately and severely mentally retarded adults to improve reaction and movement times. Am J Ment Defic. 1981;85:389-95.
- [Google Scholar]
- Training reaction and movement times of moderately and severely mentally retarded persons in aiming movements. Am J Ment Defic. 1984;89:174-9.
- [Google Scholar]
- The effect of physical fitness training on reaction time in youth with intellectual disabilities. Percept Mot Skills. 2010;111:178-86.
- [Google Scholar]
- Interhemispheric transmission time in persons with Down syndrome. J Intellect Disabil Res. 2007;51:972-81.
- [Google Scholar]
- Intracortical inhibition and facilitation with unilateral dominant, unilateral nondominant and bilateral movement tasks in left- and right-handed adults. J Neurol Sci. 2008;269:96-104.
- [Google Scholar]




