
Translate this page into:
Intraoperative diagnosis of glioblastomamultiforme with oligodendroglial and sarcomatous components
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Glioblastoma, the most frequent primary brain tumor and the most malignant neoplasm, can have the most heterogeneous morphological presentation. Along with classical morphological features, areas of oligodendroglial component and mesenchymal differentiation may be seen. The present case was a rare case of glioblastoma presenting with sarcomatous and oligodendroglial components. The case was diagnosed intraoperatively by squash and touch cytology and later on confirmed by histopathological study.
Keywords
Gliobalstoma
intraoperative
squash
touch

Introduction
Glioblastomamultiforme are high-grade malignant glial tumors of central nervous system (CNS) with divergent differentiations. According to World Health Organization nomenclature, anaplastic glial tumors with necrosis, astrocytic, and oligodendroglial components should be labeled as “glioblastoma with oligodendroglial component” and these tumors carry better prognosis than standard glioblastoma. Absence of necrosis and presence of malignant glial and oligodendroglial components, makes the tumor to be labeled as “anaplastic oligoastrocytoma”.[123]
Intraoperative cytology helps in rapid diagnosis and decision making in neurosurgical procedures. These procedures can be used as supplementary and complementary procedures to frozen section in intraoperative rapid diagnosis of CNS lesions.
We present a rare case report of glioblastoma with sarcomatous and oligodendroglial components, diagnosed by squash and touch cytology of open biopsy.
Case Report
A 60-year-old woman presented with left upper and lower limb weakness since 10 days, and headache and vomiting since 1 month. On general physical examination, no organomegaly or any lymphadenopathy was seen. On contrast-enhanced computed tomography, examination of head, a disc-enhancing lesion [Figure 1] with edema was seen in the right posterior frontal region. Per operatively a soft, firm tumor with variegated consistency and areas of bleed were seen. Part of tumor was sent to pathology department for intraoperative diagnosis in normal saline.
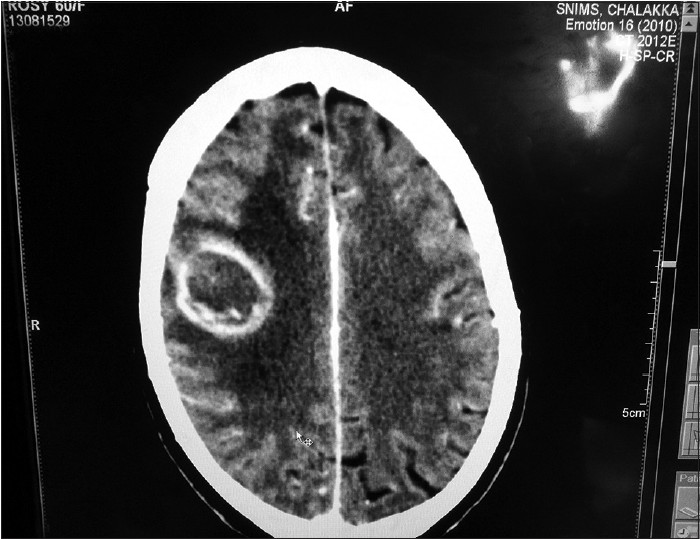
- Contrast-enhanced computed tomography examination of head displaying, a disc-enhancing lesion with edema
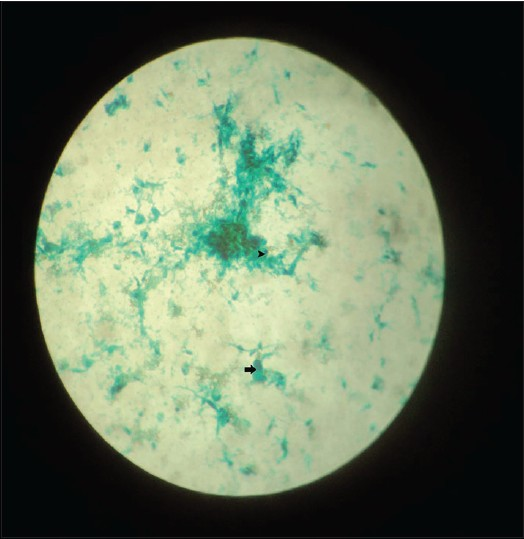
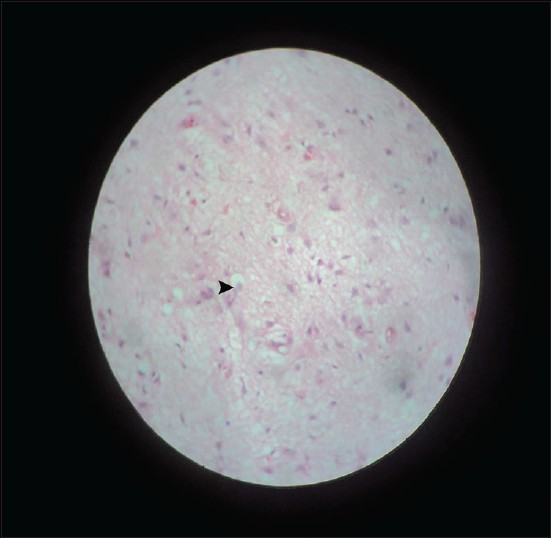
Imprint smears were prepared from tumor by touching the slide on tumor surface, and squash smears were prepared by taking a part of tumor through scalpel and keeping it between two slides and moving one slide over another, so that a thick paste comes out. Rapid hematoxylin and eosin and PAP stains were done. Microscopic examination revealed glial tissue with pleomorphic nuclei, areas of necrosis, endothelial proliferation, and areas of sarcomatous change [Figure 2] displaying interlacing bundles of spindle cells with pleomorphism. Areas of oligodendroglial tissue with small dark round nuclei and fine chromatin pattern were evident [Figure 3]. A presumptive diagnosis of “glioblastoma with sarcomatous and oligodendroglial component” was made. Subsequent biopsy examination of the remaining material confirmed the diagnosis. Reticulin stain positivity [Figure 4] was employed to confirm the diagnosis of sarcomatous component.
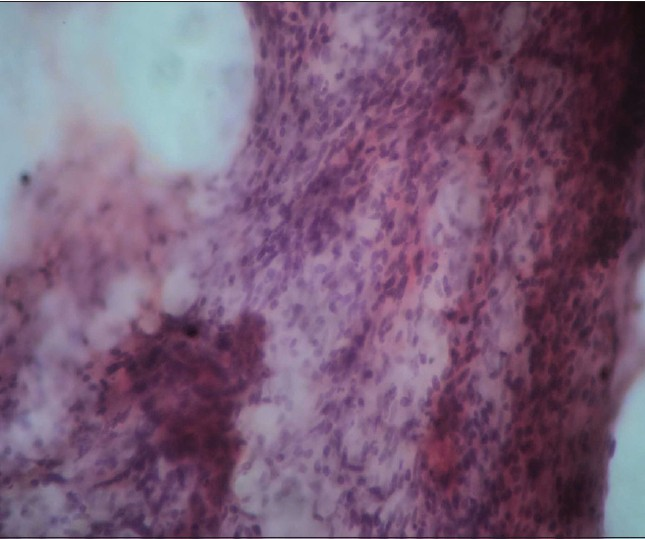
- Hematoxylin and eosin-stained squash smear, revealing tight bundles of spindle cells
- Imprint PAP-stained smear displays a round dark nuclei (arrow head) and a pleomorphic nuclei (black arrow)
- Hematoxylin and eosin-stained section displays a glial lesion with oligodendroglial component (arrow head)
Discussion
Intraoperative cytology has gained immense popularity and usefulness in diagnosis of CNS lesions, subsequent to squash technique introduction in early 1930s.[1] Cytological diagnosis of CNS lesion depends to a large extent on tissue consistency. Lesions with soft tissue consistency,[45] such as pituitary adenomas, medulloblastomas, and metastatic carcinoma pose little diagnostic problems compared with firm tissue lesions.
Gliosarcoma is a glioblastoma's variant that is characterized by biphasic pattern with areas of glial and mesenchymal differentiation.[6] The common lines of differentiation of sarcomatous components are the fibrosarcomatous and malignant fibrous histiocytoma-like types.[67] Different immunohistochemical markers showing differentiation along different components stain positive. Deposition of abundant collagen andreticulin fibers in spindle cell component by means of Masson Trichrome and reticulin staining, respectively, is helpful in clinching the diagnosis of gliosarcoma.
The present case showed varied morphological presentations of glioblastoma.
This case has to be differentiated from an oligodendroglial tumor with desmoplastic response. In the present case, separate nodule formation, predominantly composed of spindle cells is suggestive of neoplastic nature and deposition of reticulin fibers in the spindle cell components confirmed the diagnosis of gliosarcoma. Occurrence of sarcoma within oligodendroglioma is highly unusual. Similar types of reports were mentioned by Feign et al.[8] and Pasquier et al.[9] Due to its extreme rare occurrence, prognostication of tumor and response to chemotherapy regimen needs to be evaluated.
Intraoperative diagnosis of brain tumors entails frozen section and intraoperative cytology, both of which provide rapid intraoperative pathologic consultation to the neurosurgeons. Cytology samples evaluate much wider areas, which is crucial, as astrocytomas may display different grades in different areas and at different depths. Furthermore, it is easier to obtain excellent touch and squash preparation cytology than to have a high-quality brain tissue frozen section. A good cytological preparation of brain displays high cellularity, crisp nuclear and cytoplasmic details, and occasionally the tissue architecture. However, frozen sections on brain tissue may develop many artifacts, including those produced by the ice crystals and water logging in the tissues. As a result, tissue often appears smudgy, foggy, and shattered. Cytological evaluation has further advantages of being inexpensive, simple, and quicker than frozen section.
In conclusion, the tumor showed glioblastoma with sarcomatous and oligodendroglial differentiation. This unique combination describes divergent differentiation from pleuripotent stem cells. Intraoperative cytology played valuable role in diagnosis of this rare lesion.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Glioblastomas with an oligodendroglial component: A pathological and molecular study. J Neuropathol Exp Neurol. 2001;60:863-71.
- [Google Scholar]
- Correlation among pathology, genotype, and patient outcomes in glioblastoma. J Neuropathol Exp Neurol. 2006;65:846-54.
- [Google Scholar]
- Molecular genetic alterations in glioblastomas with oligodendroglial component. Acta Neuropathol. 2001;101:311-20.
- [Google Scholar]
- Smears and frozen sections in the intraoperative diagnosis of central nervous system lesions. Neurosurg Clin N Am. 1994;5:1-18.
- [Google Scholar]
- Squash preparation and frozen section in intraoperative diagnosis of central nervous system tumors. Acta Cytol. 1998;42:1149-54.
- [Google Scholar]
- Gliosarcoma. In: Kleihues P, Cavenee WK, eds. Pathology and Genetics of Tumours of the Nervous System. Lyon: IARC Press; 2000. p. :42-4.
- [Google Scholar]
- Gliosarcoma: A study of 13 tumors, including p53 and CD34 immunohistochemistry. Arch Pathol Lab Med. 1997;121:129-33.
- [Google Scholar]
- Sarcoma arising in oligodendroglioma of the brain. J Neuropathol Exp Neurol. 1976;35:679-84.
- [Google Scholar]
- Sarcoma arising in oligodendroglioma of the brain: A case with intramedullary and subarachnoid spinal metastases. Cancer. 1978;42:2753-8.
- [Google Scholar]




