
Translate this page into:
Hoffman's syndrome – A rare facet of hypothyroid myopathy
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Hoffman's syndrome is a specific, rare form of hypothyroid myopathy, which causes proximal weakness and pseudohypertrophy of muscles. It was first described in 1897 in an adult who developed muscle stiffness and difficulty in relaxation of muscles after thyroidectomy.[1] Similar presentation in children with cretinism is referred as Kocher-Debré-Sémélaigne syndrome.[2] We discuss a case of hypothyroid male with this unusual and rare presentation.
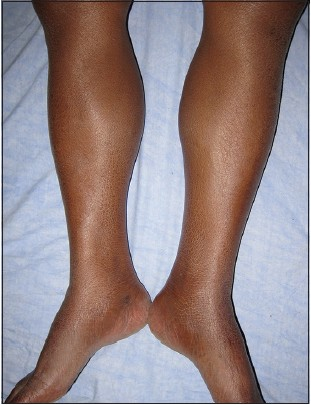
A 45-year-old male presented with complaints of weakness in lower limbs and easy fatigability for last 8 months. He had difficulty in getting up from squatting position and climbing stairs. He also complained of frequent muscular cramps and stiffness and pain in muscles. There was no history of bladder or bowel involvement. There was no history of hypertension, diabetes, or any other chronic illness. There was no history of any prolonged drug intake. On examination, he was found to have periorbital puffiness and mild pedal edema. He also had a large tongue and generalized ichthyosis. He had a pulse rate of 56/min and his blood pressure was 140/90 mm Hg. Evaluation of cardiovascular and respiratory systems did not reveal any significant abnormality. Positive findings from neurological evaluation included bilateral proximal muscle weakness in lower limbs with grade 4 power. There was hypertrophy of bilateral calf muscles (gastrocnemius) without any associated tenderness [Figures 1 and 2]. No hypertrophy of thigh, arm, or any other muscle group was noted. There was classical delayed relaxation of bilateral ankle jerks. Laboratory investigation revealed a T3 level of 0.35 ng/ml (normal range: 0.60-1.81 ng/ml), T4 level of 1.54 μg/dl (normal range: 4.5-12 μg/dl), and the activity of thyroid stimulating hormone (TSH) to be 125 μIU/ml (normal range: 0.3-5.5 μIU/ml). Anti-thyroid peroxidase (anti-TPO) antibody was positive. Creatine phosphokinase (CPK) level was 1050 IU/l (normal level: <170 U/l). Serum lactate dehydrogenase (LDH) level was slightly elevated at 235 U/l (normal range: 90-185 U/l). Hemogram revealed mild anemia. Blood sugar and liver function tests were essentially normal. Blood urea and serum creatinine were normal. Urine examination was normal and myoglobinuria was absent. Lipid profile evaluation showed hypercholesterolemia (240 mg/dl) and hypertriglyceridemia (180 mg/dl). Electrocardiography (ECG) showed low-voltage complexes and sinus bradycardia. Two-dimensional echocardiography showed mild pericardial effusion with normal systolic and diastolic functions. Nerve conduction study was normal. Electromyography showed small-amplitude myopathic motor unit potential. Based on the above findings, a diagnosis of Hoffman's syndrome was made. The patient was administered a starting dose of 100 μg/day of levothyroxine which was later escalated to 125 μg/day. On a routine follow-up later, his symptoms had improved though complete resolution of symptoms had not taken place. The calf hypertrophy, however, still persisted.

- Hypertrophy of calf muscles and associated ichthyotic skin
- Hypertrophy of calf muscles
The neurological manifestations of hypothyroidism usually occur later, and it is unusual that they are found as initial symptoms.[34] Muscular symptoms are common in hypothyroid patients (varying from myalgia, weakness, stiffness, cramps, and easy fatigability in 30-80% of the patients).[35] The common symptoms of myopathy due to hypothyroidism are proximal muscle weakness, muscle cramps, myxedema on percussion, delay in deep tendon reflexes, and rarely, development of muscle hypertrophy.[6] The muscular hypertrophy with muscle stiffness is reported in less than 10% of hypothyroid patients.[35] Although any muscle could be affected, the predominant muscles showing such changes are thigh, leg, arm, and tongue.[3] Hypertrophy of gastrocnemius is also frequently seen.[3] Similar presentation of calf muscle hypertrophy with weakness is also seen in Duchenne and Becker muscle dystrophy, focal myositis, sarcoid granulomas, and amyloid deposits in muscles. The CPK level is elevated in thyroid myopathy and is very high in some patients (10-100 times greater than the normal level); however, it has no correlation with weakness.[7] One infrequent, but potentially life-threatening complication of hypothyroid myopathy is rhabdomyolysis. It can lead to acute renal failure if not managed promptly. Some common precipitating factors are severe exercise, trauma, alcohol intake, and electrolyte imbalance.[8]
Thyroid hormones significantly influence cellular metabolism. So, their deficiency results in significant impairment of normal cellular functions. A reduction in muscle mitochondrial oxidative capacity and beta-adrenergic receptors, as well as the induction of an insulin-resistant state, may result in these changes.[6] The muscle involvement in hypothyroidism is caused by changes in muscle fibers from fast-twitching type II to slow-twitching type-I fibers.[23] This results in slowness of muscle contraction associated with hypothyroidism. The exact cause of hypertrophy remains obscure, but it could be due to an increase in connective tissue and increase in size and number of muscular fibers.[34] On histopathologic examination, the muscles appear pale and swollen. The muscle fibers may show swelling, loss of normal striations, and separation by mucinous deposits.[2] The accumulation of glycosaminoglycans in muscles could also contribute to the hypertrophy.[3] Delayed relaxation of deep tendon reflexes is due to impaired calcium sequestration by sarcoplasmic reticulum, which prolongs twitch duration.
Hypothyroidism is a very common endocrine disease and clinicians should be aware of this atypical and rare presentation of hypothyroid disease spectrum. Hoffman's syndrome represents those few forms of myopathy that completely reverse on prompt therapy and, hence, has a good outcome.
References
- Hoffmann's syndrome in hypothyroid myopathy. Report of a case in an African. Joint Bone Spine. 2001;68:84-5.
- [Google Scholar]
- The thyroid gland. In: Williams Textbook of Endocrinology (12th ed). Philadelphia: W.B. Saunders Company; 2011. p. :410.
- [Google Scholar]
- Hoffman's syndrome: Pseudohypertrophic myopathy as initial manifestation of hypothyroidism. Case report. Arq Neuropsiquiatr. 2003;61:851-4.
- [Google Scholar]
- Hypothyroidism presenting as Hoffman's syndrome. J Indian Med Assoc. 2004;102:41-2.
- [Google Scholar]
- Hypothyroid myopathy with a strikingly elevated serum creatine kinase level. Muscle Nerve. 2002;26:141-4.
- [Google Scholar]




