
Translate this page into:
Segmental schwannomatosis: An uncommon cause of crural monoparesis
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Schwannomas are nerve tumors that occur in three clinical settings – as localized schwannomas, as a part of Von Recklinghausen syndrome, or as schwannomatosis. Lower limb schwannomas are rare and can manifest with disabling pain initially. We present a case of sciatic nerve schwannoma in the setting of segmental schwannomatosis earlier misdiagnosed and treated as nonorganic until it manifested with crural weakness. A 46-year-old lady presented with intermittent low backache radiating to back of thighs and lateral aspect of calf of left lower limb of 4-year duration. She had a past history of swelling in the left calf 5 years back, which was excised and histopathology was suggestive of peripheral nerve schwannoma and she was symptom free till the onset of above symptoms. Her gadolinium enhanced magnetic resonance (MR) imaging of the lumbosacral spine including radicles (done elsewhere on more than one occasion) was normal. Three months prior to presenting to us, she experienced the dragging of left foot with repeated twisting at ankle joint and slippage of footwear along with decreased sensation over the lateral aspect of calf and foot. She had no auditory complaints and family history was noncontributory. Examination showed wasting of left thigh and calf with hypotonia. Left knee flexion was mildly weak {4/5 medical research council (MRC) grading} while ankle dorsiflexion, plantarflexion, inversion was moderately weak (2/5) with eversion being weakest (0/5). Left ankle jerk was absent. Hypoasthesia was noted over the lateral aspect of calf and dorsum as well as the plantar surface of the foot. She did not have any neurocutaneous markers. Electromyography (EMG) showed active and chronic denervation in the left tibialis anterior, gastronemius, and biceps femoris, while other muscles sampled including left lumbar, sacral paraspinal muscles, and gluteals were normal. A possibility of left sciatic nerve involvement was considered. MR imaging of sciatic nerve was done, which showed a well-defined tumour arising from the left sciatic nerve after its exit from the greater sciatic notch showing gadolinium enhancement suggestive of a sciatic nerve schwannoma [Figure 1].
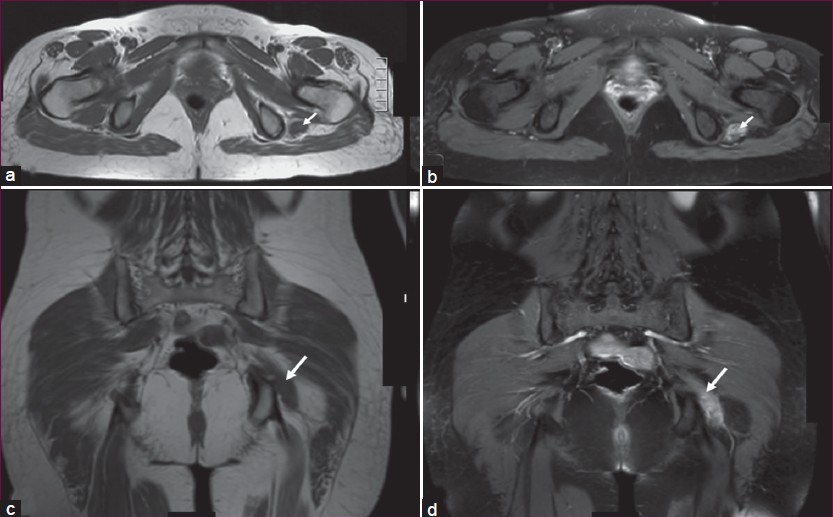
- (a) T1 axial MR section shows sciatic nerve tumour isointense to muscle measuring 4.0 × 1.6 cms, showing good enhancement post contrast (b) suggestive of a sciatic nerve schwannoma. T1 coronal MR section (c) shows the same tumour with good enhancement post contrast (d)
Schwannomas when they occur in the lower limbs are found in association with either the sciatic nerve (1%) or the posterior tibial nerve.[1] Schwannomatosis is a recently recognized third major form of neurofibromatosis (NF) and is characterized by the development of multiple schwannomas without vestibular tumors diagnostic of NF2. Our patient satisfied the criteria for possible schwannomatosis as her age was > 45 years and had two nonintradermal schwannomas, with one showing histologic confirmation and no symptoms of the eighth cranial nerve dysfunction and no known constitutional NF2 mutation.[2]
Once a subject is found to have multiple schwannomas, the possibility of NF2 must be excluded before a diagnosis of schwannomatosis is given. Most (90%) tumors in this setting have been multiple, encapsulated, and located in the subcutaneous tissue, while 10% have been plexiform, involving the neck, trunk, and extremities. Schwannomatosis may often skip generations so that more distant family members with unexplained neurological pain should be evaluated for the possibility that they are also affected. For reasons not yet understood, persons with schwannomatosis have problems with chronic pain that often exceed their neurological disability. About one-third of patients with schwannomatosis are found to have tumors in an anatomically limited distribution, such as a single limb, or < 5 contiguous segments of spine labeled as segmental schwannomatosis that affects 1/1,20,000 individuals.[2] Our patient belonged to the category of segmental schwannomatosis. Patients with schwannomatosis do not develop other types of nervous system tumors or malignancy. Schwannoma may grow up to 4 cm in diameter before symptoms arise due to nerve compression.[3] These benign tumors do not require wide area dissection or subsequent adjuvant therapy in view of their usual extreme benign course. An awareness of the existence of schwannomatosis is essential as their risk for vestibular schwannoma is nil. Schwannomatosis can present with chronic pain that often exceed their neurological disability.
Source of Support: Nil
Conflict of Interest: None declared
References
- Multiple schwannomatosis of the posterior tibial nerve. J Foot Ankle Surg. 2002;8:101-3.
- [Google Scholar]
- Schwannomas of the hand and wrist: Long-term results and review of literature. J Orthop Surg (Hong Kong). 2005;13:267-72.
- [Google Scholar]




