
Translate this page into:
Occipital dermal sinus with a vermian dermoid
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Congenital occipital dermal sinus with an underlying dermoid is a rare, benign lesion of embryological origin and may occur anywhere along the neuraxis. We present a case of a 15-year-old girl with a vermian dermoid and an occipital dermal sinus. Gross total resection of the lesion was done and post-operative period was uneventful. A detailed review of the literature is also covered.
Keywords
Congenital dermal sinus
intracranial dermoid
occipital sinus
vermian dermoid

Introduction
The dermal sinus tract is a potential communication between the skin and the deeper neural structures and present with a variety of clinical features.[1] Benign lesions of embryological origin may occur anywhere along the neuraxis, however congenital occipital dermal sinus with an underlying dermoid is rare.[1–12]
Case Report
A 15-year-old girl presented with 7 months history of intermittent occipital headaches that increased on walking, standing and was relieved by rest. There was no postural variation. She also gave a history of sustaining a road traffic accident 6 months prior to presentation after which she was apparently alright and from which she recovered uneventfully. She did not sustain any injury to the occipital region at that time. On examination, she had a small sinus in the region of the occipital protuberance with no active discharge or swelling underneath. Neurological examination was within normal limits and she did not have any cerebellar signs. MRI brain (Magnetic resonance imaging) [Figure 1] showed a well defined lesion in the region of the vermis-hypointense on T1W, hyperintense on T2W with a patchy contrast enhancement and causing compression on the vermis. Fourth ventricle was normal in shape. There was no obstructive hydrocephalus. A thin tract was seen to extend from the skin surface, coursing downwards and entering the bone just to the left of midline at the level of the torqula. A provisional diagnosis of dermoid cyst with a sinus tract was made. Other possibilities like epidermoid or dermal sinus with an assosciated abscess were also considered. She underwent midline suboccipital craniectomy and excision of the cyst. The tract was followed. It was seen to be entering the dura just below the torqula and entering into the lesion beneath. It was excised. The external surface of the lesion had a smooth, pearly appearance with small lobulations. The cyst contained cheesy, pultaceous material. Grossly, no hair follicles or other ectodermal structures were encountered. The plane between the cyst and the surrounding structures was relatively good and total resection of the cyst with the sinus tract could be achieved. Post-operatively she recovered well without any fresh deficits, seizures or aseptic meningitis. Post-operative CT scan (computed tomography) showed no residual lesion [Figure 2]. Histopathological examination of the excised cyst wall revealed a thin fibro collagenous wall with overlying stratified squamous epithelium and focal areas of bone, dystrophic calcification, cholesterol clefts and foreign body giant cells. The cyst lumen showed keratin flakes and hair shafts, suggestive of a dermoidcyst [Figure 3].
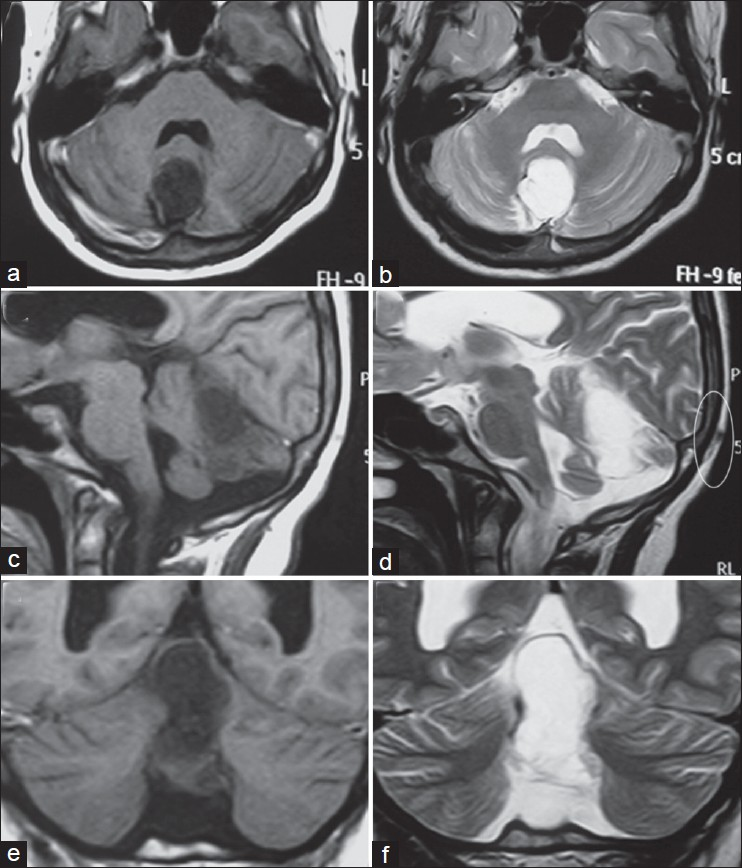
- Axial (a and b), Saggital (c and d) and Coronal (e and f) non-contrast MRI images showing a vermian lesion which is hypointense on T1W (a, c and e) and hyperintense on T2W (b, d and f). Fourth ventricle is normal in shape. A faint outline of the occipital dermal sinus tract may be made out on saggital T2W image (d, circled area)
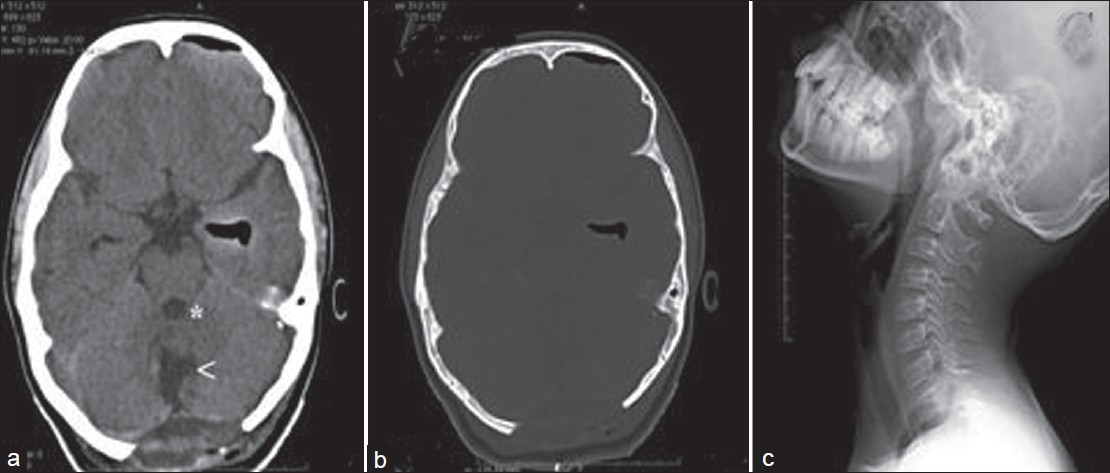
- Post-operative CT showing resection cavity (white arrow) and fourth ventricle (*) (a) and bone windows showing craniectomy defect (b). X-ray cervical spine showing no Klippel-Fiel deformity (c)
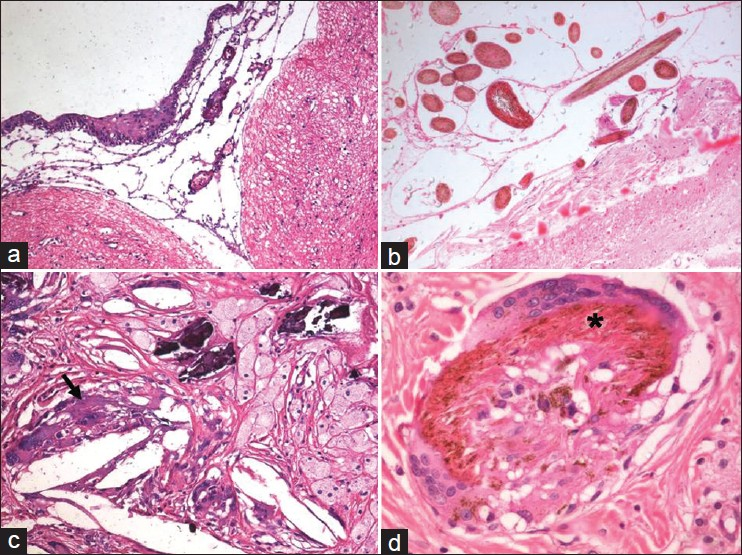
- Tissue resected shows cyst wall lined by flattened, focally stratified squamous epithelium (a) adherent to underlying gliotic cerebellar folia. Clusters of hair shaft is seen within cyst (b). There are foci of calcification, xanthogranulomatous response with giant cells, and cholesterol clefts in the cyst wall (c). Focally multinucleated giant cells are seen enclosing hair shaft (d, asterix) A:H and ExObj.10, B-D:H7ExObj.20
Discussion
Dermoid ‘tumors’ are not true neoplasms but are inclusion cysts composed of ectodermal elements. They are uncommon lesions, accounting for approximately 0.04-0.6% of all brain tumors[13–15] and are thought to arise as a result of ‘Incomplete dysjunction’ during gestation. In 60-80% of the cases, the residual tracts are associated with an inclusion tumor.[1] Dermoid cysts are well-circumscribed lesions lined by stratified squamous epithelium. They typically enlarge slowly and accumulate thick, yellowish to viscous greenish brown material that comprises of desquamated epithelium, sebaceous gland secretions, lipid metabolites, fat, oil, and whorls of hair.[1617] The presence of hair follicles and sebaceous and sweat glands in the cyst wall distinguishes dermoid from epidermoid cysts. In Wright's review of 127 cases, one fourth of the sinuses were located in the cranium and three fourths in the spine. In an elaborate review of congenital dermal sinuses by French, 85% of all cranial dermal sinuses were located at the occipital protruberance, 11% at the nasion and 5% at the posterior parietal region.[18] Of the spinal dermal sinuses, 41% were lumbar, 35% were lumbosacral, 10% were thoracic and a mere 1% were located at the cervical region.[16] Inclusion cysts associated with dermal sinus tract ended at or superficial to the dura in 18% of the cases and extended to the subdural or deeper planes in the rest.[1] Dermoid cysts have a characteristic non-homogenous appearance on imaging due to its contents. They are usually hypodense on plain CT scan and may have a negative Hounsfield unit due to the presence of fat. A thin rim of calcification is frequently present. On magnetic resonance imaging, the fat content is seen strongly hyperintense on T1W while the other contents appear hypointense. On T2W, the fat component demonstrates hypointensity similar to subcutaneous fat. Additionally, curvilinear hypointense elements may be seen if the lesion contains hair.[1131719–21] The sinus tract may not be demonstrable on MRI in all cases, thus adding to the uncertainty of diagnosis pre-operatively. Despite the rarity of lesion, the diagnosis becomes certain if a communicating tract is demonstrated on MRI, as in the present case. Occipital dermal sinus associated with a dermoid cyst may present with recurrent infections leading to meningitis or cerebellar abscesses, or with obstruction of CSF(cerebrospinal fluid) pathways due to an inclusion cyst compressing the fourth ventricle.[11622] Despite the proximity, intra-IVth ventricular inclusion cysts have only been rarely reported.[1] Dermoid cysts present as slow growing lesions with a long duration of symptoms. They may however, rarely present acutely with rupture manifesting as severe headaches, seizures, acute hydrocephalus, visual loss, aseptic meningitis or with focal neurological deficits. Imaging in such a case would demonstrate disseminated fat droplets in the sub-arachnoid space or rarely fat-fluid levels in the ventricles.[14] Some of the above features may also be seen after partial surgical removal of the cyst wall- a safe strategy to be adopted when there are dense adhesions of the capsule to the surrounding important vascular/ parenchymal structures, injury to which may lead to catastrophic complications.[14] In contrast to partially resected epidermoids, recurrence rates in partially resected dermoids are significantly less. Our case presented with non-specific headaches, probably related to minor infections in the sinus tract. Intra-operatively, there were no major adhesions and total resection of the cyst and the sinus tract could be achieved. Other associated abnormalities that have been reported include Klippel- Fiel defects. These are vertebral segmentation abnormalities leading to partial or complete fusion of multiple vertebrae. It has been described very rarely in association with posterior fossa cysts.[23] Our case, however had no associated vertebral bony anomalies.[Figure 2c].
Source of Support: Nil
Conflict of Interest: None declared
References
- Occipital dermal sinus associated with dermoid cyst in the fourth ventricle. AJNR Am J Neuroradiol. 1995;16(4 Suppl):945-8.
- [Google Scholar]
- Occipital dermal sinus: Clinical and radiological findings when a complete occipital dermal sinus is associated with a dermoid cyst. AMA J Dis Child. 1959;98:713-9.
- [Google Scholar]
- Report of eight cases of occipital dermal sinus: An update, and MRI findings. Neuropediatrics. 2001;32:153-8.
- [Google Scholar]
- Possible genetic correlation of an occipital dermal sinus in a mother and son.Case report. J Neurosurg. 2006;105(4 Suppl):326-8.
- [Google Scholar]
- Dermoid cyst of the posterior fossa associated with congenital dermal sinus in a child. World J Pediatr. 2008;4:66-9.
- [Google Scholar]
- Occipital dermal sinus associated to a cerebellar abscess.Case. Neurocirugia (Astur). 2004;15:480-3.
- [Google Scholar]
- Cerebellar dermoid cyst with occipital dermal sinus.Report of two pediatric cases. Pediatr Neurosurg. 2006;42:387-90.
- [Google Scholar]
- Occipital dermoid cyst associated with dermal sinus and cerebellar abscesses. Can J Neurol Sci. 2009;36:487-90.
- [Google Scholar]
- Mollaret meningitis associated with occipital dermal sinus. J Pediatr. 2009;155:757.e1.
- [Google Scholar]
- Prenatal diagnosis of occipital dermal sinus associated with hemangioma using ultrasound and MRI. Case report. Fetal Diagn Ther. 2006;21:232-4.
- [Google Scholar]
- Posterior fossa abscesses secondary to dermal sinus associated with dermoid cyst in children. Neuropediatrics. 2008;39:39-42.
- [Google Scholar]
- Unusual imaging appearance of an intracranial dermoid cyst. AJNR Am J Neuroradiol. 2001;22:1970-2.
- [Google Scholar]
- Ruptured intracranial dermoid cysts: Clinical, radiographic, and surgical features. Neurosurgery. 2008;62:377-84.
- [Google Scholar]
- Frontal intraparenchymal “White epidermoid cyst”: A rare occurrence. J Neurosci Rural Pract. 2011;1:125-7.
- [Google Scholar]
- Spinal congenital dermal sinuses: A 30-year experience. Pediatrics. 2003;112:641-7.
- [Google Scholar]
- Intracranial dermoid cyst mimicking a giant thrombosed aneurysm. Neurol India. 2004;52:524-5.
- [Google Scholar]
- NMR imaging of congenital intracranial germinal layer neoplasms. Neuroradiology. 1985;27:301-3.
- [Google Scholar]
- Magnetic resonance imaging and management of a pineal region dermoid. Surg Neurol. 1987;27:558-62.
- [Google Scholar]
- Diagnosis of ruptured intracranial dermoid cyst: Value MR over CT. AJNR Am J Neuroradiol. 1991;12:175-80.
- [Google Scholar]
- Congenital dermal sinuses, dermoid and epidermoid cysts of the posterior fossa. Childs Nerv Syst. 1986;2:83-9.
- [Google Scholar]
- Posterior fossa dermoid with Klippel-Feil syndrome in a child. Pediatr Neurol. 2011;45:197-9.
- [Google Scholar]




