
Translate this page into:
Primary lumbosacral intradural hydatid cyst in a child
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Primary spinal hydatid cyst is very rare lesion affecting less than 1% of the total cases of the hydatid disease. In this study, we report a case of spinal hydatid in a 5-year old boy presented with a history of backache, leg pain, difficulty in walking, and bowel and bladder incontinence for 4 months. An intradural nonenhancing cystic lesion was detected using magnetic resonance imaging from L4 to sacral region, and histopathological findings were suggestive of hydatid cyst.
Keywords
Hydatid disease
intradural
laminectomy
spinal

Introduction
Hydatid disease of the spine is caused by echinococcus granulosus. Hydatidosis of the bone occurs in 0.5-3% of all the cases reported in the literature. The vertebral column is involved in 50% of these cases. Human beings contact to the infection is by means of contamination through the direct contact with the definitive host or its faeces or by ingesting food infected with parasite. Oncospheres hatch in the duodenum, which penetrate the intestine and are carried through the bloodstream to various organs.[1] Spinal hydatid cysts account for 1% of all cases of hydatid disease.[1] Primary spinal intradural hydatid cysts are very rare. The disease usually spreads over the spine by the direct extension from abdominal, pulmonary, or pelvic manifestation and most commonly affects the thoracic region of the spine. In this study, we report a case of intradural hydatid cyst of lumbosacral region in a child which is extremely rare.
Case Report
A 5-year-old boy presented with a history of gradually increasing backache, pain in both lower limbs, and difficulty in walking for 4 months. Later, he developed urinary and faecal incontinence. Neurological examination revealed paraparesis of lower motor neuron type and diminished sensation below L4 on both sides with loss of perianal sensation. Anal tone was decreased. Power was 2/5 in both lower limbs. Knee and ankle jerk were absent and plantars were nonelicitible.
The magnetic resonance imaging (MRI) of lumbosacaral spine revealed well-defined intradural cystic lesions from L4 to sacral region. There were cerebrospinal fluid (CSF) like intensities on T1 - and T2 -weighted images. No contrast enhancement was observed. Ultrasonography of abdomen, chest X-ray, and serological tests (ELISA-IGg) were negative for any systemic foci.
The patient underwent L4 to S1 laminectomy. An intradural cystic lesion was removed totally with capsule, and the cavity was irrigated with hypertonic saline [Figure 1]. Histopathological examination confirmed the presence of hydatid cyst [Figure 2]. Postoperative period was uneventful. Albendazole 10 mg/kg was given for a period of 3 months. Although there was complete regain of sensation in 3-4 weeks, motor function and bladder control recovered only after 4 months.
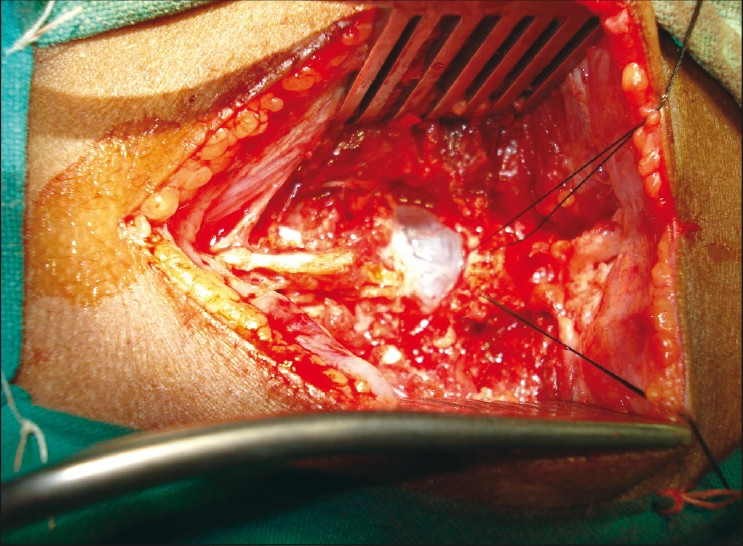
- Intra-operative photograph showing the detail of hydatid cyst
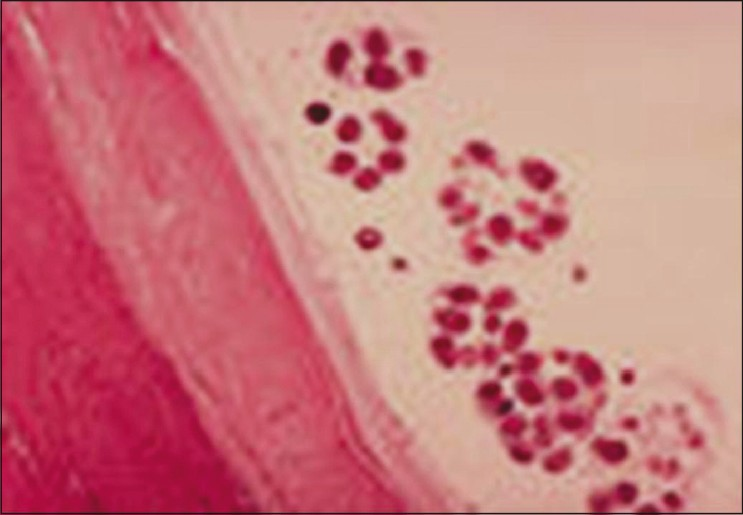
- Histopathological examination confi rmed the presence of hydatid cyst (H and E, ×40).
Discussion
Hydatid disease is generally caused by an infection by echinococcus granulomsus and prevalent in most of sheep-raising regions of the world.[1] Spinal hydatid cysts account for 1% of all cases of hydatid disease.[1] The disease usually spreads over the spine by direct extension from abdominal, pulmonary, or pelvic infection, and most commonly affects the dorsal region of the spine. Spinal hydatid cysts are located most commonly at the thoracic (52%), followed by the lumbar (37%), and then the sacral.
Primary spinal intradural hydatid cyst is extremely rare.[1] In the most recent reviews by Chakir et al.,[2] 23 cases of intradural spinal hydatid cysts were reported in the literature. In another recent study, Hilmani et al.[3] reported a case of intradural hydatid cyst. Similarly Kahilogullari et al.[1] also reported a case. All these 25 cases were reported in adults.
Recently, Kalkan et al.[4] reported a case of intradural hydatid cyst in a child in dorsal region. To the best of our knowledge, the present study is the first case of primary intradural hydatid cyst in a child in lumbosacral region in the literature.
Clinically spinal echinococcus manifests by radicular pain associated with objective sensory and motor disturbances and local tenderness at the level of the involved vertebra. There are no pathognomic signs and symptoms of this disease. Because of these features, it is often misdiagnosed initially as tuberculosis of the spine, spinal tumor, or disc prolapse.
Recurrence remains a major problem in spinal hydatidosis; the literature cites rates of 30-100%. Because of high recurrence rate, spinal hydatidosis has a poor prognosis. On MRI examination, hydatid cysts appear as well-circumscribed, cystic lesions, with CSF-like signal intensities. The cyst wall is usually thin and regular with no septations. The cysts are hypotense on T1W images and hyperintense on T2W images. No contrast enhancement is seen [Figures 3 and 4].

- Sagittal T1W MRI showing cystic well-defi ned lesion from L4 to sacral region
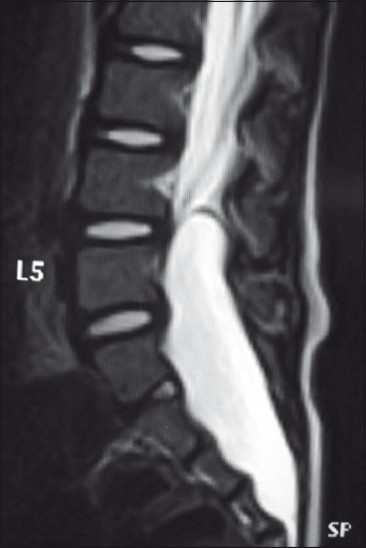
- Sagittal T1W MRI showing hyperintense cystic lesion from L4 to sacral region.
The choice of treatment in spinal hydatid disease is the laminectomy and total removal of the cysts without rupture. Irrigating the wound with hypertonic saline or diluted betadine solution after the cyst removal helps destroy and disrupt the parasites. In the early postoperative period, adjuvant antihelminthic drug therapy must be given for at least 3 months.
Conclusion
Although primary intradural hydatid cyst was very rare, it was the documented cause of backache, leg pain, gait disturbance and urinary and faecal incontinence in this child. MRI is the investigation of choice, and the best treatment is total surgical excision without rupture. High rate of recurrence is a major problem, and this can be reduced by total resection of the cyst with its capsule without rupture and the administration of antihelminthic drugs.
Source of Support: Nil,
Conflict of Interest: None declared.
References
- Primary intradural extramedullary hydatidosis.Case report and review of the literature. J Neuroradiol. 2002;29:177-82.
- [Google Scholar]
- Primary spinal intradural extramedullary hydatid cyst in a child. J Spinal Cord Med. 2007;30:297-300.
- [Google Scholar]




